


Abstract
Blastomycosis is an endemic dimorphic fungal infection that most commonly involves the lungs and may disseminate to extrapulmonary sites, particularly the skin. Central nervous system (CNS) involvement is uncommon and is estimated to occur in approximately 5–10% of disseminated cases, most often as meningitis, meningoencephalitis, or parenchymal abscesses. Sellar or pituitary involvement is exceptionally rare and has been described primarily in isolated case reports. We present a previously healthy man who presented with neurological findings. Imaging demonstrated a sellar/suprasellar lesion and scattered pulmonary densities. We review the challenges of diagnosis and treatment of this rare presentation of blastomycosis.
Highlights
- Disseminated blastomycosis can rarely involve the pituitary gland and present with hypopituitarism.
- Central nervous system involvement occurs in a minority of disseminated cases and may mimic neoplasm in imaging.
- Bronchoscopy or biopsy of a verrucous cutaneous lesion can provide an accessible diagnostic target when sellar biopsy is high risk.
- Liposomal amphotericin B followed by an azole with CNS penetration (e.g., voriconazole) is standard therapy for CNS disease.
1. Introduction
Blastomycosis is a systemic pyogranulomatous infection caused by the dimorphic fungus Blastomyces dermatitidis. It is endemic to regions of North America, including the Ohio and Mississippi River valleys and the Great Lakes basin [1,2].
Infection typically begins after inhalation of conidia with primary pulmonary involvement; hematogenous dissemination may occur to extrapulmonary sites such as skin, bone, and the genitourinary tract [1,2]. CNS involvement is uncommon, occurring in approximately 5–10% of disseminated blastomycosis, and it may present as meningitis, meningoencephalitis, or parenchymal brain abscesses [3–5].
Pituitary involvement by blastomycosis is exceptionally rare and may be mistaken for more common sellar processes such as pituitary adenoma, hypophysitis, metastasis, or craniopharyngioma [6–8]. We report a case of disseminated blastomycosis in an otherwise healthy man presenting with hypopituitarism due to pituitary involvement, and we discuss the diagnostic value of classic cutaneous lesions as an alternative biopsy target.
2. Case Presentation
A 48-year-old previously healthy man presented with a two-week history of progressive headaches, dizziness, blurred vision, and polyuria with polydipsia. He denied fever, weight loss, cough, or recent travel. His medical history was unremarkable, and he reported no chronic medications. He was born in Serbia and immigrated to the United States 10 years prior with no subsequent travel abroad. He worked in construction, reported smoking 1.5 packs of cigarettes daily, and denied illicit drug use, significant alcohol consumption, known tuberculosis exposure, or owning household pets.
Upon presentation, he had a low-grade temperature of 99.1 °F with otherwise normal vital signs. Physical examination demonstrated coarse breath sounds over the right lung fields. Neurologic examination was notable for visual disturbances without focal motor deficits. Dermatologic examination identified a raised, scaly plaque on the left wrist (Figure 1).
Initial laboratory studies showed a white blood cell count of 9.3 ˆ 109/L and hyponatremia with a sodium level of 121 mmol/L. The remaining electrolytes, creatinine, and liver function tests were within normal limits.
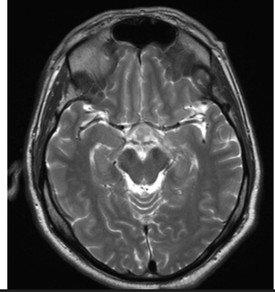
Computed tomography (CT) of the head demonstrated a poorly defined hypodense lesion in the medial temporal lobe with mild enlargement of the pituitary gland. Subsequent magnetic resonance imaging (MRI) of the brain revealed an enhancing lesion involving the pituitary gland with extension into the sella as well as suprasellar and infrasellar regions, including involvement of the optic chiasm (Figure 2). Given concern for disseminated disease, CT imaging of the chest was obtained and demonstrated scattered bilateral pulmonary densities with a focal rounded infiltrate in the right lower lobe (Figure 3).
Lumbar puncture revealed a cerebrospinal fluid (CSF) white blood cell count of 43 cells/μL with lymphocytic predominance (70%), an elevated protein level of 76 mg/dL, and a normal glucose level of 74 mg/dL. CSF cultures and polymerase chain reaction testing were negative.
Endocrine evaluation demonstrated hypopituitarism, including central hypothyroidism, diabetes insipidus, and secondary adrenal insufficiency. Hormone replacement therapy was initiated with desmopressin, prednisone, and levothyroxine. Bronchoscopy with transbronchial biopsy was subsequently performed, and fungal cultures grew Blastomyces dermatitidis, confirming disseminated blastomycosis.
The patient was initiated on liposomal amphotericin B; however, therapy was discontinued after two weeks due to the development of acute kidney injury. During the two-week interval, he demonstrated marked clinical improvement with a resolution of headaches and improvement in visual and urinary symptoms. Repeat MRI showed a significant decrease in the size of the enhancing sellar lesion with a complete resolution of previously noted infra- and supratentorial foci, consistent with treatment response (Figure 4). He was transitioned to oral voriconazole for long-term antifungal therapy.
3. Discussion
3.1. Epidemiology and Frequency of CNS Involvement
Blastomycosis is an endemic dimorphic fungal infection caused by Blastomyces dermatitidis. Endemic regions in North America include the Ohio and Mississippi River valleys and the Great Lakes basin [1,2]. Primary infection typically involves the lungs after inhalation of conidia, with subsequent dissemination via hematogenous spread in a subset of patients [1,2].
CNS involvement is uncommon but clinically important. Across guidelines and modern series, CNS disease has been estimated to occur in approximately 5–10% of disseminated blastomycosis [3–5]. Reported presentations include chronic meningitis, meningoencephalitis, and parenchymal lesions such as abscesses. Accordingly, disseminated blastomycosis with CNS involvement should be considered rare relative to pulmonary and cutaneous disease, yet it carries substantial morbidity and often presents with nonspecific symptoms and imaging findings [3–5].
3.2. Pituitary Involvement and Infectious Mimics of Sellar Masses
Pituitary involvement by blastomycosis is exceptionally rare, with only isolated case reports describing sellar disease complicated by hypopituitarism [6,7]. As in the present case, symptoms may include headaches, visual disturbances from optic chiasm involvement, and endocrine dysfunction such as diabetes insipidus and central adrenal or thyroid insufficiency [6,7].
The differential diagnosis of an enhancing sellar/suprasellar lesion is broad, and infectious etiologies can closely mimic neoplasm. Sellar lesions mimicking pituitary adenomas have been described, and clinical-radiographic correlation is essential [9]. Bacterial pituitary abscesses are an important consideration and may present headaches, visual symptoms, and hypopituitarism; diagnosis often requires a combination of imaging and microbiologic/histopathologic confirmation [9, 10]. Fungal infection of the pituitary region is rare but has been reported, including pituitary fungal granulomas [11]. Broader reviews of infections affecting the hypothalamic–pituitary region emphasize that tuberculosis and other granulomatous infections can also cause hypopituitarism and diabetes insipidus, particularly in patients with compatible epidemiologic risk [12].
3.3. Cutaneous Manifestations and the Diagnostic Value of Skin Biopsy
Cutaneous involvement is among the most common extrapulmonary manifestations of disseminated blastomycosis and may provide a readily accessible diagnostic target [2]. Classic cutaneous lesions are often verrucous or ulcerative plaques with raised, heaped-up borders and a scaly or crusted surface, and they may clinically resemble squamous cell carcinoma or other chronic inflammatory dermatoses [2].
The raised, scaly plaque observed on this patient’s left wrist (Figure 1) was consistent with these classic descriptions. When such lesions are present, an early dermatologic evaluation of lesions with biopsy can expedite diagnosis and may obviate the need for higher-risk procedures (e.g., sellar biopsy) [2,7]. In particular, a biopsy taken from the active edge of the heaped-up border can improve diagnostic yield because the advancing inflammatory margin is more likely to contain organisms and diagnostic histopathology [2]. Histopathology typically demonstrates broad-based budding yeasts with thick, refractile walls, and fungal culture provides definitive identification [1,2].
3.4. Cerebrospinal Fluid Studies and Adjunctive Testing
CSF findings in CNS blastomycosis are frequently nonspecific and can overlap with other infectious and inflammatory processes. Typical CSF profiles include lymphocytic pleocytosis and elevated protein with low-to-normal glucose [3,4]. CSF cultures may have limited sensitivity, and diagnosis often depends on the identification of Blastomyces from tissue or culture at another involved site [4]. Antigen testing (e.g., urine, serum, or CSF when available) can support the diagnosis in disseminated disease, but results must be interpreted in clinical context because cross-reactivity with other endemic fungi has been described [1,4].
3.5. Treatment Considerations for CNS and Sellar Disease
The management of CNS blastomycosis requires prolonged antifungal therapy. Infectious Diseases Society of America guidelines recommend induction therapy with a lipid formulation of amphotericin B for CNS disease, followed by prolonged oral azole therapy for at least 12 months and until clinical and radiographic resolution [3]. Azole selection for CNS disease is influenced by CNS penetration and activity against blastomycosis; voriconazole has been used successfully in CNS blastomycosis and is often favored when enhanced CNS bioavailability is desired or when amphotericin B is not tolerated [4,13].
In the present case, the patient received liposomal amphotericin B with rapid clinical and radiographic improvement but required early discontinuation due to acute kidney injury. Transition to voriconazole was therefore appropriate, given the need for long-term therapy and CNS penetration [3,4,13]. Because pituitary involvement may result in persistent endocrinopathies, careful assessment and management of adrenal insufficiency, diabetes insipidus, and thyroid dysfunction are critical during treatment and follow-up [6,12].
4. Conclusion
Pituitary involvement in disseminated blastomycosis is exceptionally rare but can present with hypopituitarism and diabetes insipidus [6,7]. Disseminated blastomycosis with CNS involvement remains uncommon overall, occurring in an estimated 5–10% of disseminated cases [3,4]. Recognition of classic cutaneous lesions and consideration of early skin biopsy—preferably at the active edge of a heaped-up border—may provide a safe and high-yield diagnostic approach when sellar tissue sampling is high risk [2,9]. The timely initiation of guideline-directed therapy with amphotericin B followed by prolonged azole therapy, along with appropriate endocrine replacement, is essential to optimize neurologic and endocrine outcomes [3,4,12].
Funding
This research received no external funding.
Acknowledgments
The author used ChatGPT for content assistance, specifically to create an initial draft from prior personal presented material. The manuscript was reviewed and revised the material generated and takes full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Saccente, M.; Woods, G.L. Clinical and laboratory update on blastomycosis. Clin. Microbiol. Rev. 2010, 23, 367–381. [CrossRef] [PubMed]
- McBride, J.A.; Gauthier, G.M.; Klein, B.S. Clinical Manifestations and Treatment of Blastomycosis. Clin. Chest Med. 2017, 38, 435–449. [CrossRef] [PubMed]
- Chapman, S.W.; Dismukes, W.E.; Proia, L.A.; Bradsher, R.W.; Pappas, P.G.; Threlkeld, M.G.; Kauffman, C.A. Clinical practice guidelines for the management of blastomycosis: 2008 update by the infectious diseases society of America. Clin. Infect. Dis. 2008, 46, 1801–1812. [CrossRef] [PubMed]
- Bariola, J.R.; Perry, P.; Pappas, P.G.; Proia, L.; Shealey, W.; Wright, P.W.; Sizemore, J.M.; Robinson, M.; Bradsher, R.W. Blastomycosis of the central nervous system: A multicenter review of diagnosis and treatment in the modern era. Clin. Infect. Dis. 2010, 50, 797–804. [CrossRef] [PubMed]
- Ryan, D.; Lippert, W.C.; Fenwick, A.J.; Bhatt, M.; Jones, C.R. Central Nervous System Blastomycosis with Multiple Brain Abscesses Presenting as Right Upper Extremity Weakness. Neurohospitalist 2019, 9, 230–234. [CrossRef] [PubMed]
- Abrams, E.; Dean, H.J.; Bunge, M.K.; Taback, S.P.; Sellers, E.A.C. Blastomycosis of the central nervous system in a child: A rare cause of hypopituitarism. J. Pediatr. Endocrinol. Metab. 2011, 24, 775–777. [CrossRef] [PubMed]
- Morse, H.G.; Nichol, W.P.; Cook, D.M.; Blank, N.K.; Ward, T.T. Central nervous system and genitourinary blastomycosis: Confusion with tuberculosis. West. J. Med. 1983, 139, 99–103. [PubMed]
- Karmarkar, V.S.; Deopujari, C.E. Sellar Pathologies Mimicking Pituitary Tumors. Neurol. India 2020, 68, S154–S160. [CrossRef] [PubMed]
- Vates, G.E.; Berger, M.S.; Wilson, C.B. Diagnosis and management of pituitary abscess: A review of twenty-four cases. J. Neurosurg. 2001, 95, 233–241. [CrossRef] [PubMed]
- Karagiannis, A.K.; Dimitropoulou, F.; Papatheodorou, A.; Lyra, S.; Seretis, A.; Vryonidou, A. Pituitary abscess: A case report and review of the literature. Endocrinol. Diabetes Metab. Case Rep. 2016, 2016, 160014. [CrossRef] [PubMed]
- Jain, K.C.; Varma, A.; Mahapatra, A.K. Pituitary abscess: A series of six cases. Br. J. Neurosurg. 1997, 11, 139–143. [CrossRef] [PubMed]
- Pekic, S.; Miljic, D.; Popovic, V. Infections of the Hypothalamic-Pituitary Region. In Endotext ; Feingold, K.R., Adler, R.A., Ahmed, S.F., Anawalt, B., Blackman, M.R., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 27 September 2024.
- Bakleh, M.; Aksamit, A.J.; Tleyjeh, I.M.; Marshall, W.F. Successful treatment of cerebral blastomycosis with voriconazole. Clin. Infect. Dis. 2005, 40, e69–e71. [CrossRef] [PubMed]