Abstract
Pelvic actinomycosis is an uncommon chronic infection most frequently associated with prolonged intrauterine device (IUD) use. We present the case of a 42-year-old woman with no history of IUD use who developed a pelvic abscess six weeks following an uncomplicated robotic total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO) performed for endometriosis. Eventual imaging demonstrated a 7 cm gas- and fluid-containing collection within the surgical bed consistent with abscess formation. Interventional radiology-guided percutaneous drainage culture yielded Actinomyces species, establishing the diagnosis of pelvic actinomycosis. The patient was treated with targeted antimicrobial therapy and source control with clinical improvement. This case highlights the importance of considering actinomycosis in the differential diagnosis of post-surgical pelvic collections, even in the absence of traditional risk factors such as IUD use, and underscores the role of prolonged antimicrobial therapy in achieving durable clinical cure.
Highlights
- Pelvic actinomycosis is an uncommon but clinically significant infection most frequently associated with prolonged intrauterine device (IUD) use, though it can occur following gynecologic surgery even in the absence of IUD history.
- Actinomyces species are anaerobic or microaerophilic Gram-positive rods that cause chronic, progressive infection characterized by abscess formation, fibrosis, draining sinus tracts, and fistulae following mucosal barrier disruption.
- Pelvic actinomycosis is frequently misdiagnosed as a gynecologic malignancy or tubo-ovarian abscess, leading to unnecessary surgical intervention and delayed antimicrobial therapy.
- Definitive treatment requires prolonged antibiotic therapy, typically comprising intravenous beta-lactams for 2–6 weeks followed by oral suppressive therapy for 6–12 months, in combination with source control when indicated.
- Co-pathogens including anaerobes, streptococci, staphylococci, and Enterobacterales commonly accompany Actinomyces and should be addressed in empirical antimicrobial selection.
1. Introduction
Actinomycosis is a chronic, progressive bacterial infection caused by Actinomyces species, which are filamentous anaerobic or microaerophilic Gram-positive rods that are normal commensals of the oropharyngeal, gastrointestinal, and genitourinary mucosa [1–4]. Infection develops when mucosal barrier integrity is disrupted, allowing bacterial invasion into deeper tissues. The organism then incites a characteristic inflammatory response featuring granulomatous tissue formation, reactive fibrosis, abscess development, draining sinus tracts, and fistulae [1–4]. The pathogenesis is typically polymicrobial, with co-pathogens—including anaerobes, Staphylococcus spp., Streptococcus spp., and Enterobacterales—contributing to tissue invasion by inhibiting host defenses and lowering local oxygen tension [1–4].
2. Case Presentation
A 42-year-old woman with a past medical history significant for endometriosis underwent an uncomplicated robotic total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO). She had no prior history of intrauterine device use and no significant prior hospitalizations or recurrent antibiotic exposures.
Her initial postoperative course was unremarkable. However, approximately three weeks postoperatively, she developed progressive shortness of breath and was admitted to an outside hospital where bilateral pleural effusions were identified. Thoracentesis demonstrated exudative fluid; cultures were negative, and no infectious etiology was identified. She was empirically treated with ceftriaxone and metronidazole. A repeat thoracentesis 1 week later was similarly unremarkable for a bacterial process, and she was discharged on a corticosteroid taper.
Approximately six weeks postoperatively (two weeks after her hospital discharge and four days prior to her subsequent admission), the patient began noticing vaginal discharge, which became malodorous one day prior to presentation. She reported mild pelvic discomfort but denied fevers, chills, night sweats, rash, or weight loss. She was directed to the emergency department by the on-call gynecologist.
On examination, the patient was hemodynamically stable with a temperature of 37.2 °C, heart rate of 100 beats per minute, blood pressure of 114/67 mmHg, and respiratory rate of 16 breaths per minute. She was alert and oriented, in no acute distress. The abdomen was soft and non-distended with minimal tenderness to palpation. The remainder of the physical examination, including cardiovascular, pulmonary, musculoskeletal, and dermatologic assessments, was unremarkable.
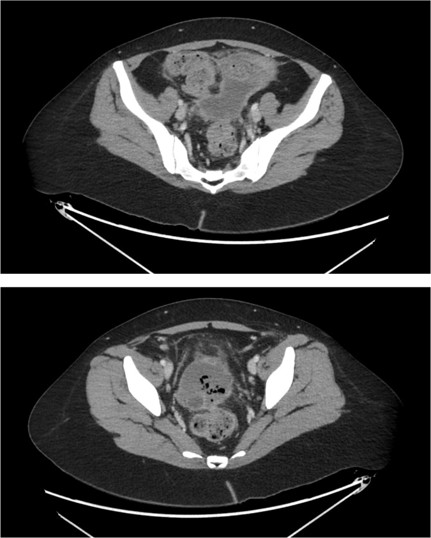
Computed tomography (CT) of the abdomen and pelvis revealed a large gas- and fluid-containing collection within the post-hysterectomy surgical bed measuring up to 7 cm, which is highly concerning for abscess formation (Figure 1). There was an extension of phlegmonous changes to adjacent bowel loops, including the small and large bowel within the pelvis and the appendix, with circumferential bowel wall thickening likely secondary to regional inflammatory changes. Diffuse thickening of the bladder wall was also noted, likely reactive in nature. No obvious intra-abdominal perforation was identified.
Interventional radiology-guided percutaneous drainage was performed. Gram stain of the aspirate demonstrated Gram-negative rods as well as Gram-positive cocci in pairs, chains, and clusters. The patient was initiated on broad-spectrum empirical antimicrobial therapy.
Subsequent culture results identified heavy growth of Actinomyces species, establishing the diagnosis of pelvic actinomycosis. The patient was transitioned to targeted intravenous (IV) antimicrobial therapy with ertapenem directed against both the Actinomyces and the identified co-pathogens (Peptostreptococcus sp. and Finegoldia magna), with plans for prolonged oral suppressive therapy with amoxicillin–clavulanate following completion of the IV induction phase.
3. Discussion
3.1. Pathogenesis and Predisposing Factors
Actinomycosis develops when Actinomyces species breach the mucosal barrier and invade deeper tissues, inciting a chronic inflammatory response characterized by granulomatous tissue formation with central necrosis, progressive fibrosis, abscess formation, draining sinus tracts, and fistulae. This process is facilitated by co-pathogens—including anaerobes, Staphylococcus spp., Streptococcus spp., and Enterobacterales—that inhibit local host defenses and reduce oxygen tension, creating a microenvironment conducive to Actinomyces proliferation [1–4].
Recognized predisposing factors for actinomycosis include diabetes mellitus, immunosuppression, malnutrition, and local tissue damage or inflammation [1–4]. In the pelvic setting, prolonged IUD use is the most frequently cited risk factor, reported in approximately 75% of cases in some series. The mechanism is thought to involve chronic low-grade endometrial inflammation and microtrauma associated with the foreign body, creating a portal of entry for commensal organisms [3–5].
In the present case, the patient had no history of IUD use or other traditional predisposing factors aside from the recent surgical disruption of pelvic tissues. Robotic TAHBSO, while minimally invasive, still involves extensive dissection of the uterine and adnexal pedicles and vaginal cuff closure, creating tissue planes susceptible to colonization by endogenous flora. The surgical breach of the cervicovaginal mucosal barrier likely provided the portal of entry for Actinomyces species resident in the lower genital tract.
3.2. Clinical Manifestations and Disease Patterns
Actinomycosis is classified by anatomic site into four principal forms: orocervicofacial, thoracopulmonary, abdominal, and pelvic (Table 1). Orocervicofacial disease is the most common, typically following dental procedures or maxillofacial trauma. Thoracopulmonary actinomycosis may develop after aspiration or extension from cervicofacial disease. Abdominal disease most commonly follows appendicitis, diverticulitis, or abdominal surgery [1–4]. Pelvic actinomycosis accounts for a significant minority of cases and is most strongly associated with prolonged intrauterine device (IUD) use, reported in up to 75% of cases in some series [3–5]. Other predisposing factors include diabetes mellitus, immunosuppression, malnutrition, and local tissue damage or inflammation [1–4].
| Clinical Form | Key Features |
|---|---|
| Orocervicofacial | Most common form; cervicofacial mass, draining sinus tracts following dental procedures, oral surgery, or maxillofacial trauma |
| Thoracopulmonary | Pulmonary consolidation, chest wall invasion, and sinus tracts; may follow aspiration or extend from cervicofacial disease |
| Abdominal | Post-appendicitis, post-diverticulitis, or post-surgical; presents as mass lesion or abscess mimicking malignancy |
| Pelvic | Most commonly associated with IUD use; lower abdominal pain, vaginal discharge/bleeding; frequently misdiagnosed as gynecologic malignancy or tubo-ovarian abscess |
Pelvic actinomycosis presents a diagnostic challenge because its clinical and radiographic features frequently mimic gynecologic malignancy or tubo-ovarian abscess, leading to misdiagnosis and, in some cases, unnecessary radical surgical intervention [3–6]. The infection may present as either a slowly progressive, non-tender, indurated mass or as acute suppurative disease [1–4]. Clinical features typically include lower abdominal pain, vaginal bleeding or discharge, and constitutional symptoms including fever, weight loss, and fatigue [3–6].
Reports of pelvic actinomycosis following total abdominal hysterectomy with bilateral salpingo-oophorectomy (TAH-BSO) in the absence of IUD history are limited in the literature, making recognition of this entity in the post-surgical setting particularly important [5,6].
The patient in this case presented with a relatively late onset of infection following surgical disruption, with abscess formation identified on cross-sectional imaging. The polymicrobial Gram stain findings including Gram-negative rods with Gram-positive cocci in pairs, chains, and clusters were consistent with the mixed flora typical of actinomycotic infections. It does not appear that the exudative pleural effusions diagnosed and treated in the previous hospitalization were infectious; rather, these were likely inflammatory from retro-peritoneal dissection during the original surgery [7].
3.3. Diagnostic Considerations
The diagnosis of actinomycosis is frequently delayed due to its rarity, indolent course, and propensity to mimic other conditions [1–4]. Microbiologic diagnosis is challenging because Actinomyces species are fastidious, slow-growing organisms that may be obscured by faster-growing co-pathogens in polymicrobial cultures [1–4]. Prolonged anaerobic culture incubation (up to 14–21 days) may be required for isolation [1–4]. Histopathologic identification of characteristic sulfur granule colonies of Actinomyces organisms within inflammatory tissue can support the diagnosis when culture results are equivocal [1–4].
Cross-sectional imaging with CT characteristically demonstrates a solid mass or complex cystic collection with surrounding inflammatory changes, often with extension across tissue planes—a finding that, while not pathognomonic, should raise clinical suspicion in the appropriate context [3–6]. In this case, the CT findings of a gas- and fluid-containing pelvic collection with phlegmonous extension to adjacent bowel and appendix prompted appropriate interventional drainage and microbiologic sampling, ultimately yielding the diagnosis.
3.4. Treatment Considerations
The cornerstone of actinomycosis treatment is prolonged antimicrobial therapy, often in combination with surgical source control when abscesses, fistulae, or extensive necrotic tissue are present. Actinomyces species demonstrate excellent susceptibility to beta-lactam antibiotics, which form the backbone of treatment [1–4,8].
For monopathogen actinomycosis, preferred intravenous agents include penicillin G, ampicillin, or ceftriaxone. When polymicrobial infection is documented or suspected, as is typical in pelvic actinomycosis, broader-spectrum regimens such as piperacillin–tazobactam or carbapenems are appropriate to provide coverage of both Actinomyces and co-pathogens (Table 2). The recommended treatment paradigm consists of an intravenous induction phase of 2–6 weeks, followed by oral suppressive therapy for 6–12 months, or at a minimum of 2 months beyond clinical and radiographic resolution of infection. Oral step-down options include amoxicillin, penicillin V, or doxycycline [1–4,7]. Treatment of the co-pathogens in the oral suppressive therapy period is likely not necessary.
| Phase | Monopathogen | Polymicrobial/Co-Pathogen |
|---|---|---|
| IV Induction (2–6 weeks) | IV penicillin G, ampicillin, or ceftriaxone | Piperacillin–tazobactam or carbapenems |
| Oral Suppression (6–12 months) | Amoxicillin, penicillin V, or doxycycline | Amoxicillin, penicillin V, or doxycycline (with co-pathogen coverage as indicated) |
Source control through surgical debridement or percutaneous drainage is an important adjunct, particularly in the setting of large abscesses or undrained collections [1–4]. In the present case, interventional radiology-guided percutaneous drainage provided effective source control and facilitated microbiologic diagnosis. One should continue to monitor the development of recurrent abscess or fistula formation between the GI and GU tract.
3.5. Pelvic Actinomycosis After Hysterectomy
While the association between pelvic actinomycosis and IUD use is well-established, reports of actinomycosis following TAH-BSO in the absence of IUD history are limited in the literature [5,6]. Choi et al. described a case series emphasizing the diagnostic confusion between pelvic actinomycosis and gynecologic malignancy, while Ferjaoui et al. reported a case of pelvic actinomycosis mimicking an ovarian tumor in a post-surgical setting [5,6]. These reports collectively underscore that any disruption of pelvic mucosal integrity, whether from foreign body, surgery, or local inflammation, can predispose to actinomycotic infection.
The present case adds to this limited body of literature by demonstrating that robotic TAH-BSO, despite its minimally invasive approach, can create sufficient tissue disruption to facilitate Actinomyces invasion. Clinicians should maintain a high index of suspicion for actinomycosis in patients presenting with post-surgical pelvic collections that fail to respond to conventional antimicrobial therapy or that demonstrate atypical features on imaging.
4. Conclusions
Pelvic actinomycosis is an uncommon but clinically important infection that is most frequently associated with prolonged IUD use but can also develop following gynecologic surgery in the absence of traditional risk factors [1–6]. This case illustrates that robotic TAH-BSO, despite its minimally invasive nature, can provide sufficient mucosal disruption to facilitate Actinomyces invasion and subsequent pelvic abscess formation.
Clinicians should maintain actinomycosis in the differential diagnosis of post-surgical pelvic collections that demonstrate atypical features, fail to respond to conventional antimicrobial therapy, or yield polymicrobial cultures with unexpected organisms. A deliberate approach incorporating prolonged anaerobic culture incubation, cross-sectional imaging, source control, and extended antimicrobial therapy-typically, 2–6 weeks of intravenous beta-lactam induction followed by 6–12 months of oral suppressive therapy-is essential for achieving a durable clinical cure and preventing relapse [1–4,8].
Funding
This research received no external funding.
Acknowledgments
The author used Claude for content assistance, specifically to create an initial draft from prior personal presented material. The manuscript was reviewed and the author revised the material generated and takes full responsibility for the content of this publication.
Conflicts of Interest
The author declares no conflict of interest.
References
- Wong, V.K.; Turmezei, T.D.; Weston, V.C. Actinomycosis. BMJ 2011, 343, d6099. [CrossRef]
- Valour, F.; Sénéchal, A.; Dupieux, C.; Karsenty, J.; Lustig, S.; Breton, P.; Gleizal, A.; Boussel, L.; Laurent, F.; Braun, E.; et al. Actinomycosis: Etiology, clinical features, diagnosis, treatment, and management. Infect. Drug. Resist. 2014, 7, 183–197. [CrossRef]
- Bonnefond, S.; Catroux, M.; Melenotte, C.; Karkowski, L.; Rolland, L.; Trouillier, S.; Raffray, L. Clinical features of actinomycosis: A retrospective, multicenter study of 28 cases of miscellaneous presentations. Medicine 2016, 95, e3923. [CrossRef]
- Brook, I. Actinomycosis: Diagnosis and management. South Med. J. 2008, 101, 1019–1023. [CrossRef] [PubMed]
- Choi, S.E.; Kwon, J.H.; Park, S.H.; Koh, S.B. A case of pelvic and abdominal actinomycosis after hysterectomy. Korean J. Obstet. Gynecol. 2007, 50, 1586–1590.
- Ferjaoui, M.A.; Arfaoui, R.; Khedhri, S.; Hannechi, M.A.; Abdessamia, K.; Samaali, K.; Fezai, W.; Salhi, M.; Malek, M.; Neji, K. Pelvic actinomycosis: A confusing diagnosis. Int. J. Surg. Case Rep. 2021, 86, 106387. [CrossRef]
- Yu, J.; Park, J.-Y.; Kim, D.-H.; Kim, S.; Hwang, J.-H.; Seo, H.; Kim, Y.-K. Incidence and Risk Factors of Pulmonary Compilations after Robot-assisted Laparoscopic Prostatectomy: A Retrospective Observational Analysis of 2208 Patients at a Large Single Center. J. Clin. Med. 2019, 8, 1509. [CrossRef] [PubMed] [PubMed Central]
- Hsueh, L.; Singh, A. The destructive potential of penile actinomycosis: A case report. Priv. Pract. Infect. Dis. 2024, 4, 10. [CrossRef]