Abstract
Methicillin-susceptible Staphylococcus aureus (MSSA) bacteremia is commonly treated with beta-lactam antibiotics, including cefazolin and antistaphylococcal penicillins. Although cefazolin is supported as first-line therapy for MSSA bacteremia, management of high-inoculum endovascular infections remains challenging, and persistent bacteremia may occur despite apparent susceptibility. We describe a 24-year-old man with a history of recurrent skin boils who presented with progressive facial swelling and high-grade MSSA bacteremia complicated by cavernous sinus thrombosis, septic venous thrombophlebitis, septic pulmonary emboli, and subsequent mycotic aneurysm with subarachnoid hemorrhage. Blood cultures remained persistently positive despite cefazolin monotherapy, raising concern for a high-inoculum endovascular infection and a possible cefazolin inoculum effect. Escalation to cefazolin plus ertapenem was associated with clearance of bacteremia, and the patient ultimately completed a prolonged course of cefazolin with clinical improvement after neurovascular intervention. This case highlights the limitations of cefazolin monotherapy in severe MSSA infections involving protected endovascular sites. In addition to aggressive diagnostic evaluation and source control, consideration of antimicrobial pharmacodynamics and the use of synergistic beta-lactam therapy may be warranted in refractory cases.
Highlights
- Persistent MSSA bacteremia despite cefazolin should prompt reassessment for high-inoculum endovascular infection and adequacy of source control.
- The cefazolin inoculum effect is not detected by routine susceptibility testing and may be clinically relevant in select high-burden infections.
- Short-course dual beta-lactam therapy (e.g., cefazolin plus ertapenem) has been used as salvage therapy to clear refractory MSSA bacteremia.
- Intracranial vascular complications such as mycotic aneurysm and subarachnoid hemorrhage require urgent multidisciplinary evaluation and intervention.
1. Introduction
MSSA bacteremia is commonly treated with β-lactam antibiotics, including cefazolin and antistaphylococcal penicillins. While cefazolin is supported by clinical data as first-line therapy, management of high-inoculum endovascular infections remains challenging, and persistent bacteremia may occur despite apparent susceptibility [1–5].
We report a young man with invasive MSSA bacteremia complicated by cavernous sinus thrombosis, septic pulmonary emboli, and intracranial vascular complications who required salvage dual beta-lactam therapy for microbiologic clearance.
2. Case Presentation
A 24-year-old man with a past medical history significant for latent tuberculosis infection and recurrent skin abscesses presented with progressive facial swelling, shortness of breath, and fevers. Several days prior to presentation, he reported scratching the inside of his nose, resulting in a possible minor cut. The following day, he developed fevers and chills, followed by worsening nasal and facial swelling. He initially sought care at an urgent care clinic, where he was diagnosed with influenza and prescribed oseltamivir, along with amoxicillin–clavulanate for presumptive bacterial sinusitis. Despite two days of outpatient therapy, his symptoms progressed with the development of right-sided chest discomfort, increasing shortness of breath, and worsening facial swelling, prompting hospital evaluation.
On presentation, the patient appeared toxic and diaphoretic. His temperature was 99.3 °F,
his blood pressure was 158/107 mm Hg, his heart rate was 112 bpm, his respiratory rate was 31, and he was saturating 97% on room air. Physical examination revealed marked nasal swelling with multiple furuncles, erythema and edema of the nasal and periorbital tissues, bilateral sinus swelling, and proptosis. Extraocular movements were limited in all directions. There was no photophobia or nuchal rigidity. Cardiovascular examination demonstrated tachycardia without murmurs. Pulmonary examination was notable for diffuse rhonchi and associated conversational dyspnea. The abdominal examination was soft and non-tender, and no peripheral edema or rash was observed.
Laboratory evaluation demonstrated significant leukocytosis with a white blood cell count of 20.4 ˆ 109/L and neutrophilic predominance (87%). Hemoglobin was 15.8 g/dL and platelet count was 236 ˆ 109/L. Severe hyponatremia was noted with a sodium level of 114 mmol/L. Renal function was preserved with a blood urea nitrogen of 8 mg/dL and creatinine of 0.64 mg/dL. Mild transaminitis was present with an aspartate aminotransferase of 46 U/L and alanine aminotransferase of 82 U/L. Procalcitonin was markedly elevated at 8.2 ng/mL.
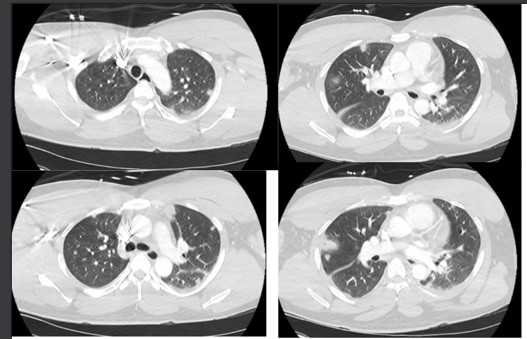
Initial chest radiography demonstrated increased interstitial markings and a 2.0 ˆ 2.0 cm nodular opacity in the right lung. Computed tomography (CT) of the head showed no evidence of acute intracranial hemorrhage, mass effect, or midline shift but revealed bilateral periorbital and premaxillary soft-tissue swelling, with fluid and inflammatory stranding within the intraorbital regions, greater on the left, concerning for orbital and post-septal cellulitis. CT of the chest demonstrated multiple bilateral nodular and ground-glass opacities, several with central cavitation, consistent with septic pulmonary emboli (Figure 1).
With the concern of intracranial extension, magnetic resonance venography of the brain was obtained and demonstrated bilateral cavernous sinus thrombosis with extension into the superior ophthalmic veins. Additional findings included bilateral orbital cellulitis with a 2.0 ˆ 0.9 cm non-enhancing collection in the right retrobulbar region contiguous with the right superior ophthalmic vein, suspicious for abscess. Extensive superficial thrombophlebitis was noted, involving the bilateral orbital veins, bifrontal, periorbital, and perinasal superficial veins, and left premaxillary veins. Nonocclusive thrombi were identified in the inferior petrosal sinuses with extension into the upper internal jugular veins, proximal jugular veins, and superior sagittal sinus. Mild bilateral dural enhancement was present without significant leptomeningeal enhancement.
Given the severity of orbital involvement, ophthalmology was urgently consulted and noted tense eyelids, bilateral proptosis with chemosis, and severely limited extraocular movements in all fields of gaze. Bilateral canthotomies were performed for orbital decompression. Otolaryngology evaluated the patient and performed nasal endoscopy, which did not reveal purulence or mass lesions. Due to concern for intracranial extension, the patient was transferred to a tertiary care center for neurosurgical evaluation, where an initial cerebral angiogram did not demonstrate vascular abnormalities.
Blood cultures obtained on admission grew MSSA by BioFire molecular testing. The patient was initially treated with linezolid and ceftriaxone while awaiting final susceptibility testing, then de-escalated to cefazolin alone. Blood cultures remained persistently positive for MSSA on hospital days 1, 2, and 3.
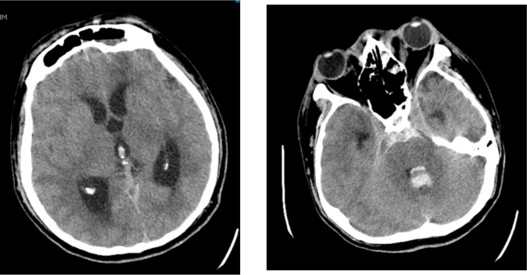
On hospital day 4, the patient developed worsening headache, confusion, and fever to 101.8 °F. Repeat computed tomography of the head demonstrated new extensive subarachnoid hemorrhage involving the basilar cisterns with extension into the third and fourth ventricles and dependent portions of the lateral ventricles, as well as extension into the upper cervical spinal canal. Interval dilation of the lateral, third, and fourth ventricles was noted, consistent with acute hydrocephalus (Figure 2). An external ventricular drain was emergently placed.
Given persistent high-grade bacteremia and concern for a high-inoculum endovascular infection with central nervous system involvement, antimicrobial therapy was escalated to cefazolin plus ertapenem for salvage therapy. Following this change, the MSSA cleared from his bloodstream the subsequent day. Evaluation for underlying immunodeficiency, including HIV testing, quantitative immunoglobulins, and IgG subclasses, was unremarkable. Transesophageal echocardiography did not demonstrate evidence of infective endocarditis. The septic pulmonary emboli were suspected to have propagated from the bilateral internal jugular vein thrombosis.
The hospital course was further complicated by the development of loculated pleural effusions requiring drainage with a right-sided chest tube. Otolaryngology subsequently performed sinus washout. Repeat cerebral angiography following an intracranial hemorrhage identified a left anterior inferior cerebellar artery mycotic aneurysm, which was successfully treated with endovascular coiling. The hospital course was further complicated by a seizure, leading to discontinuation of ertapenem 1 week later. Patient was continued on cefazolin monotherapy to complete 6 weeks of treatment from clearance of bacteremia with significant clinical improvement.
3. Discussion
This case illustrates a rare but life-threatening presentation of MSSA bacteremia complicated by extensive endovascular and intracranial vascular involvement, including cavernous sinus thrombosis, mycotic aneurysm formation, and septic pulmonary emboli. While MSSA bacteremia is common, persistent bacteremia with progression of endovascular disease despite guideline-concordant therapy highlights the importance of pathogen-specific, infection-site-specific, and inoculum-dependent considerations in antimicrobial selection.
3.1. First-Line Beta-Lactam Therapy for MSSA Bacteremia
Beta-lactam antibiotics remain the cornerstone of therapy for MSSA bacteremia. Antistaphylococcal penicillins (ASPs), such as oxacillin and nafcillin, have historically been considered first-line agents due to their stability against staphylococcal β-lactamases and extensive clinical experience in deep-seated infections. However, cefazolin has emerged as a preferred alternative in many settings due to favorable tolerability and comparable efficacy [6,7]. The CloCeBa randomized trial demonstrated cefazolin to be non-inferior to cloxacillin for the treatment of MSSA bacteremia overall, with fewer adverse events in the cefazolin arm [1].
Notably, exploratory subgroup analyses from CloCeBa suggested potential heterogeneity of treatment effect based on blaZ genotype. Among patients infected with MSSA isolates harboring blaZ type I β-lactamase, cefazolin did not meet the prespecified criteria for non-inferiority compared with cloxacillin, whereas non-inferiority was maintained in infections caused by other blaZ genotypes [1]. Although this subgroup analysis was not powered to detect definitive differences in clinical outcomes, these findings raise the possibility that β-lactamase-mediated hydrolysis may influence cefazolin performance in select high-risk settings and are biologically consistent with prior mechanistic and in vitro data examining the cefazolin inoculum effect [2].
3.2. The Cefazolin Inoculum Effect and High-Inoculum Endovascular Infection
β-lactam selection in high-inoculum MSSA infections remains nuanced. One potential limitation of cefazolin is the cefazolin inoculum effect (CzIE)—a phenomenon in which cefazolin minimum inhibitory concentrations increase substantially at high bacterial densities. This effect is mediated by hydrolysis of cefazolin by certain staphylococcal β-lactamases, most notably those encoded by blaZ type A and, less consistently, type C alleles. In contrast, ASPs are relatively resistant to these enzymes, which has historically supported their preferential use in infections characterized by high bacterial burden, such as endocarditis and deep endovascular infections.
The clinical relevance of the cefazolin inoculum effect remains controversial. Several observational studies and systematic reviews have failed to demonstrate a consistent association between CzIE and increased mortality or treatment failure in patients treated with cefazolin for MSSA bacteremia. A recent comprehensive analysis published in Clinical Infectious Diseases found that, although CzIE is biologically plausible and detectable in vitro, its presence has not been reliably associated with inferior clinical outcomes in most cohorts, particularly when appropriate source control is achieved [2]. In this patient, after source control was obtained, he was de-escalated back to cefazolin monotherapy. Importantly, standard clinical microbiology testing does not detect CzIE, as cefazolin susceptibility is inferred from oxacillin or cefoxitin testing, limiting the ability to prospectively identify affected isolates.
Nevertheless, the CzIE remains a clinically relevant consideration in select scenarios, particularly in patients with persistent bacteremia or extensive endovascular infection despite appropriate therapy. High-grade bacteremia involving thrombosed venous sinuses, septic thrombi, or vascular lesions represents an environment in which bacterial burden may be sufficiently high for inoculum-dependent pharmacodynamic limitations to become clinically meaningful. In such cases, lack of early microbiologic clearance may warrant reassessment of antimicrobial strategy even in the absence of formal resistance.
In the present case, persistent high-grade MSSA bacteremia occurred despite cefazolin therapy in the setting of extensive endovascular disease. Notably, there was no concern for inadequate central nervous system penetration of cefazolin. Recent pharmacokinetic and clinical data demonstrate that cefazolin achieves therapeutic concentrations within inflamed meningeal and intracranial tissues, and
CNS involvement alone should not be considered a limitation to its use in MSSA infections [2]. Instead, concern centered on the possibility of a high-inoculum, β-lactamase-mediated effect limiting cefazolin efficacy within endovascular compartments, particularly in the absence of immediate source control.
3.3. Salvage Dual Beta-Lactam Therapy for Persistent MSSA Bacteremia
Combination β-lactam therapy has emerged as a salvage strategy in such refractory cases. Multiple clinical series have demonstrated rapid clearance of persistent MSSA bacteremia following the addition of ertapenem to cefazolin, likely due to synergistic inhibition of complementary penicillin-binding proteins and enhanced activity against high-burden infections [3–5]. In vitro biofilm models further support the efficacy of this combination, demonstrating potent bactericidal activity against MSSA within structured biofilms and endovascular analogues [4,5].
In this patient, escalation to cefazolin plus ertapenem was associated with prompt clearance of bacteremia, supporting the growing body of literature suggesting that combination β-lactam therapy may overcome inoculum-related pharmacodynamic limitations in refractory MSSA infections. While ertapenem was later discontinued due to seizure activity, microbiologic clearance had already been achieved, and cefazolin monotherapy was successfully continued thereafter.
3.4. Cavernous Sinus Thrombosis and Intracranial Vascular Complications
This case also underscores the potential for nasal and facial soft-tissue infection to extend into the cavernous sinus via valveless venous pathways, resulting in septic thrombosis, orbital involvement, and downstream septic embolization. Rapid recognition and early cross-sectional imaging (including venous imaging when indicated) are essential to define disease extent and guide urgent specialty interventions.
Progression to subarachnoid hemorrhage with identification of a mycotic aneurysm highlights that ongoing bacteremia and intracranial venous thrombosis can be accompanied by arterial complications. In patients with neurologic deterioration or hemorrhage, prompt neurocritical care and repeat vascular imaging may be required to identify treatable lesions and prevent catastrophic rebleeding.
3.5. Key Educational Takeaways
This case underscores several important clinical principles. Persistent MSSA bacteremia should prompt reassessment of antimicrobial pharmacodynamics and infection burden. Cefazolin remains an effective first-line agent for MSSA bacteremia, including infections with CNS involvement, but clinicians should remain alert to scenarios in which high bacterial burden or endovascular disease may limit cefazolin monotherapy effectiveness. Finally, combination β-lactam therapy represents a reasonable salvage strategy in refractory cases, though prospective studies are needed to better define patient selection, optimal duration, and long-term outcomes.
4. Conclusions
Invasive MSSA bacteremia involving protected endovascular and intracranial vascular sites can persist despite guideline-concordant cefazolin therapy. When bacteremia fails to clear promptly, clinicians should reassess for uncontrolled infection burden and consider whether inoculum-dependent pharmacodynamics could be contributing. In select refractory cases, short-course dual beta-lactam therapy (such as cefazolin plus ertapenem) may provide a salvage option to achieve rapid microbiologic clearance, followed by completion of definitive therapy with a standard first-line agent.
Funding
This research received no external funding.
Acknowledgments
The authors used Claude for content assistance, specifically to create an initial draft from prior personal presented material. The manuscript was reviewed and the authors revised the material generated and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Burdet, C.; Saïdani, N.; Dupieux, C.; Lemaignen, A.; Surgers, L.; Vareil, M.O.; Lepeule, R.; Charmillon, A.; Le Moing, V.; Boutoille, D.; et al. Cloxacillin versus cefazolin for methicillin-susceptible Staphylococcus aureus bacteraemia (CloCeBa): A prospective, open-label, multicentre, non-inferiority, randomised clinical trial. Lancet 2025, 406, 2349–2359. [CrossRef] [PubMed]
- Pitcock, C.; Burgess, D.S.; Olney, K.B. Optimizing cefazolin dosing for central nervous system infections: Insights from population pharmacokinetics and Monte Carlo simulations. Antimicrob. Agents Chemother. 2025, 69, e0185724. [CrossRef] [PubMed]
- Ulloa, E.R.; Singh, K.V.; Geriak, M.; Haddad, F.; E Murray, B.; Nizet, V.; Sakoulas, G. Cefazolin and Ertapenem Salvage Therapy Rapidly Clears Persistent Methicillin-Susceptible Staphylococcus aureus Bacteremia. Clin. Infect. Dis. 2020, 71, 1413–1418. [CrossRef] [PubMed]
- Gilbertie, J.; Ulloa, E.R.; Daiker, J.C.; Nguyen, K.; Smelter, D.; Rose, W.; Geriak, M.; Schnabel, L.V.; Nizet, V.; Sakoulas, G. Potent Activity of Ertapenem Plus Cefazolin Within Staphylococcal Biofilms: A Contributing Factor in the Treatment of Methicillin-Susceptible Staphylococcus aureus Endocarditis. Open. Forum Infect. Dis. 2022, 9, ofac159. [CrossRef] [PubMed]
- Sakoulas, G.; Olson, J.; Yim, J.; Singh, N.B.; Kumaraswamy, M.; Quach, D.T.; Rybak, M.J.; Pogliano, J.; Nizet, V. Cefazolin and Ertapenem, a Synergistic Combination Used To Clear Persistent Staphylococcus aureus Bacteremia. Antimicrob. Agents Chemother. 2016, 60, 6609–6618. [CrossRef] [PubMed]
- Prosty, C.; Noutsios, D.; Lee, T.C.; Daneman, N.; Davis, J.S.; Jager, N.G.; Ghanem-Zoubi, N.; Goodman, A.L.; Kaasch, A.J.; Kouijzer, I.; et al. Cefazolin vs. antistaphylococcal penicillins for the treatment of methicillin-susceptible Staphylococcus aureus bacteraemia: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2025, 31, 1272–1282. [CrossRef] [PubMed]
- Jaime-Ardila, L.J.; Támara-Rivera, J.L.; Nocua-Báez, L.C.; Díaz-Brochero, C.; Melendez-Rhenals, S.D.M. Comparative effectiveness of cefazolin versus antistaphylococcal penicillins in methicillin-susceptible Staphylococcus aureus infective endocarditis: A systematic review of observational studies. Ther. Adv. Infect. Dis. 2025, 12, 20499361251384146. [CrossRef] [PubMed]