Multiple myeloma
Review this module to better understand infectious complications in patients with multiple myeloma and associated therapy.
20%
1 / 5
1. 49 yo woman with PMH relapsed refractory IgG Lamba Multiple Myeloma, most recently treated with Isatuximab, Pomalyst, dexamethasone presents to the hospital with 3 days of altered mental status, fevers, generalized malaise and CXR shows a dense left lower lobe consolidation. Based off her underlying disease, prior treatments and clinical presentation, what is the most likely diagnosis?
Explanation : Answer: B. Bacterial infection/pneumonia with an encapsulated organism.
Blood cultures grew out Streptococcus pneumoniae. This patient is most likely to have a bacterial infection/pneumonia with an encapsulated organism. Patients with multiple myeloma have a decrease in CD19+ B cells and reduced ability to secrete polyclonal immunoglobulins and ability to differentiate into Ab secreting plasma cells, which predisposes patients to infections with encapsulated organisms.
Reference: Diaz-Tegedor A, Lorenzo-Mohamed M, Paino T et al. Mechanisms and Therapeutic Strategies to Reverse Immunosuppression. Cancers 2021, 13 (6), 1353. DOI:10.3390/cancers13061353
Reference: Diaz-Tegedor A, Lorenzo-Mohamed M, Paino T et al. Mechanisms and Therapeutic Strategies to Reverse Immunosuppression. Cancers 2021, 13 (6), 1353. DOI:10.3390/cancers13061353
40%
2 / 5
2. What strategy would you use to reduce the risk of this type of infection in this patient?
Explanation : Answer: D. All of the above. Vaccination with the conjugated vaccine (PCV13, PCV 15) followed by the polysaccharide PPV 23 after 2 months or an even longer interval is recommended. If the conjugated PCV20 vaccine is used, a dose of PPV23 is not indicated. A retrospective study in Clinical Lymphoma, Myeloma & Leukemia showed that IVIG was effective at preventing infectious events in patients with non-progressive disease multiple myeloma with hypogammaglobulinemia. Antibiotic prophylaxis during periods of neutropenia is recommended.
References:
Lancman G, Lozada K, Chari A et al. Efficacy of Intravenous Immunoglobulin for Preventing Infections in Patients with Multiple Myeloma. Clinical Lymphoma, Myeloma & Leukemia, Vol 21, No. 5 e470-6. DOI: 10.1016/j.clml.2020.12.026
Ludwig H, Boccadoro M, Moreau P, Sonneveld P et al. Recommendations for Vaccination in Multiple Myeloma: A Consensus of the European Multiple Myeloma Network. Leukemia (2021) 35:31-44. DOI: 10.1038/s41375-020-01016-0
References:
Lancman G, Lozada K, Chari A et al. Efficacy of Intravenous Immunoglobulin for Preventing Infections in Patients with Multiple Myeloma. Clinical Lymphoma, Myeloma & Leukemia, Vol 21, No. 5 e470-6. DOI: 10.1016/j.clml.2020.12.026
Ludwig H, Boccadoro M, Moreau P, Sonneveld P et al. Recommendations for Vaccination in Multiple Myeloma: A Consensus of the European Multiple Myeloma Network. Leukemia (2021) 35:31-44. DOI: 10.1038/s41375-020-01016-0
60%
3 / 5
3. With Bortezomib, what type of infection is 4X more likely compared to treatment with high dose dexamethasone?
Explanation : Answer: B. Varicella Zoster infection
Bortezomib causes decrease in T cell proliferation as well as decreased function of NK and CD8 cells. It has been associated with 4X higher incidence of Varicella zoster infection in newly diagnosed patients compared to high dose dexamethasone. Prophylaxis with acyclovir or valacyclovir is recommended in patients receiving Bortezomib.
Reference:
Nucci M, Anaissie E. Infections in Patients with Multiple Myeloma in the Era of High-Dose Therapy and Novel Agents. CID 2209; 49-1211-25. DOI: 10.1086/605664
Reference:
Nucci M, Anaissie E. Infections in Patients with Multiple Myeloma in the Era of High-Dose Therapy and Novel Agents. CID 2209; 49-1211-25. DOI: 10.1086/605664
80%
4 / 5
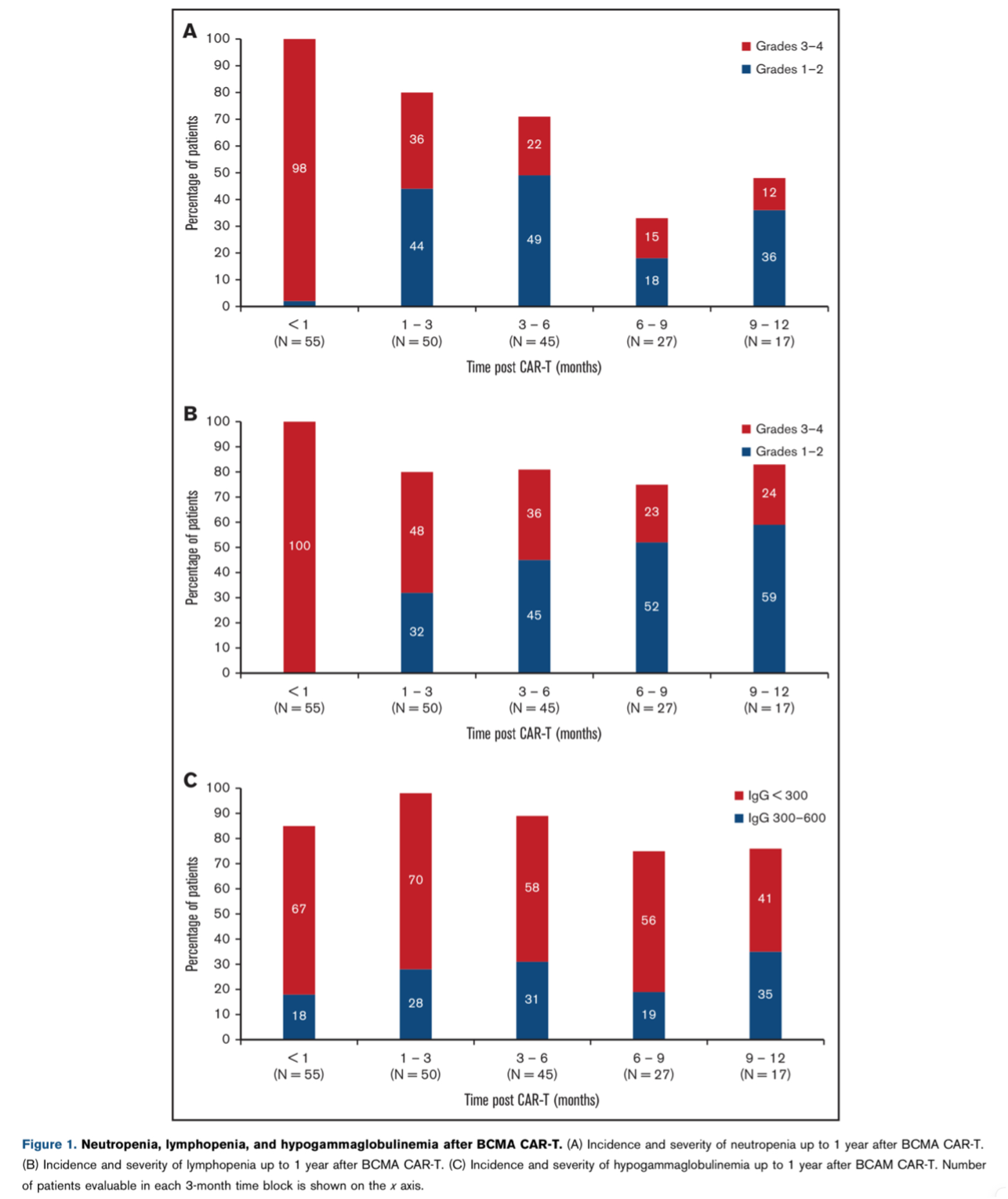
4. One year post BCMA CAR-T cell therapy for relapsed multiple myeloma, what percentage of patients have persistent hypogammaglobulinemia?
Explanation : Answer: C. ~75%
In a single center retrospective analysis of infection outcomes at UCSF up to 1 year after BCMA CAR-T cell therapy for MM, 76% had persistent hypogammaglobulinemia 1 year post CAR-T cells.

Reference:
Kambhampati S, Sheng Y, Wong S et al. Infectious Complications in Patients with Relapsed Refractory Multiple Myeloma after BCMA CAR T cell therapy. Blood advances. Blood Adv. 2022 Apr 12; 6 (7): 2045-2054. DOI: 10.1182/bloodadvances.2020004079
Reference:
Kambhampati S, Sheng Y, Wong S et al. Infectious Complications in Patients with Relapsed Refractory Multiple Myeloma after BCMA CAR T cell therapy. Blood advances. Blood Adv. 2022 Apr 12; 6 (7): 2045-2054. DOI: 10.1182/bloodadvances.2020004079
100%
5 / 5
5. During the early pre-engraftment period post autologous SCT for multiple myeloma, of the following options, which infection is the most likely?
Explanation : Answer: B. Bacterial infections/complications related to mucositis
During the pre-engraftment period post autologous transplant for multiple myeloma, patients typically have infectious complications related to neutropenia and mucositis. Pneumocystis pneumonia and CMV are typically characterized by decreased cell mediated immunity which occurs later in the post engraftment period. Mold infections with invasive aspergillosis are more common with prolonged periods neutropenia and allogeneic hematopoietic stem cell transplant recipients.
Reference:
Nucci M, Anaissie E. Infections in Patients with Multiple Myeloma in the Era of High-Dose Therapy and Novel Agents. CID 2209; 49-1211-25. DOI: 10.1086/605664
Reference:
Nucci M, Anaissie E. Infections in Patients with Multiple Myeloma in the Era of High-Dose Therapy and Novel Agents. CID 2209; 49-1211-25. DOI: 10.1086/605664